
Page 63 - Revista Portuguesa - SPORL - Vol 52 Nº3
P. 63
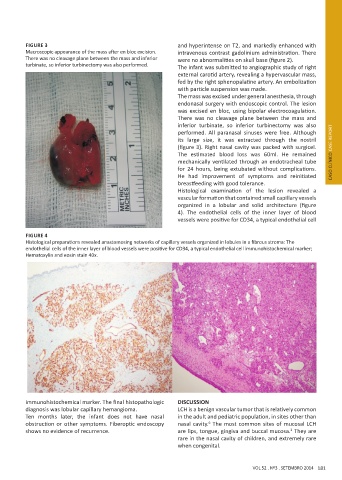
FIGURE 3 and hyperintense on T2, and markedly enhanced with
Macroscopic appearance of the mass after en bloc excision. intravenous contrast gadolinium administration. There
There was no cleavage plane between the mass and inferior were no abnormalities on skull base (figure 2).
turbinate, so inferior turbinectomy was also performed. The infant was submitted to angiographic study of right
external carotid artery, revealing a hypervascular mass,
fed by the right sphenopalatine artery. An embolization
with particle suspension was made.
The mass was excised under general anesthesia, through
endonasal surgery with endoscopic control. The lesion
was excised en bloc, using bipolar electrocoagulation.
There was no cleavage plane between the mass and
inferior turbinate, so inferior turbinectomy was also
performed. All paranasal sinuses were free. Although
its large size, it was extracted through the nostril
(figure 3). Right nasal cavity was packed with surgicel.
The estimated blood loss was 60ml. He remained CASO CLÍNICO CASE REPORT
mechanically ventilated through an endotracheal tube
for 24 hours, being extubated without complications.
He had improvement of symptoms and reinitiated
breastfeeding with good tolerance.
Histological examination of the lesion revealed a
vascular formation that contained small capillary vessels
organized in a lobular and solid architecture (figure
4). The endothelial cells of the inner layer of blood
vessels were positive for CD34, a typical endothelial cell
FIGURE 4
Histological preparations revealed anastomosing networks of capillary vessels organized in lobules in a fibrous stroma: The
endothelial cells of the inner layer of blood vessels were positive for CD34, a typical endothelial cell immunohistochemical marker;
Hematoxylin and eosin stain 40x.
immunohistochemical marker. The final histopathologic DISCUSSION
diagnosis was lobular capillary hemangioma. LCH is a benign vascular tumor that is relatively common
Ten months later, the infant does not have nasal in the adult and pediatric population, in sites other than
obstruction or other symptoms. Fiberoptic endoscopy nasal cavity. The most common sites of mucosal LCH
6
shows no evidence of recurrence. are lips, tongue, gingiva and buccal mucosa. They are
2
rare in the nasal cavity of children, and extremely rare
when congenital.
VOL 52 . Nº3 . SETEMBRO 2014 181